Live Tides
NOTICES TO MARINERS
Charts & Surveys
Incident reporting
Life-threatening emergencies on the river:
Call 999 and ask for the Coastguard
For near miss, safety observations and incident reporting click below

Incident investigations, reports and data
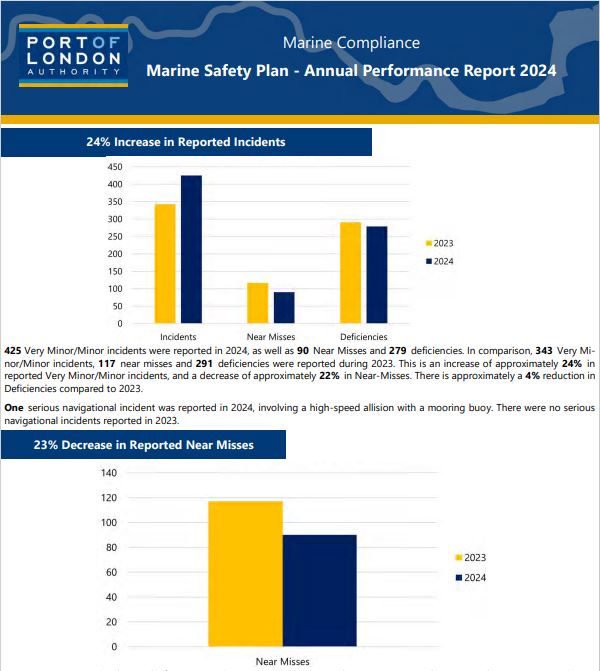
The Port of London's Authority's Marine Management Team (MMM) regularly reviews the Safety Management System's (SMS) performance against our three yearly Marine Safety Plan
 Performance reports
Performance reportsThe latest quarterly and annual SMS reports which contain these SMS reviews as well as incident statistics.
Six Monthly Reports
Annual Reports
For any questions regarding the above reports please contact the Marine Compliance Team at [email protected]
Summary of navigational incidents in the Port of London
An Integral part of the port's Marine Safety Management System involves the investigation of all navigational incidents that are reported to the Harbour Master. Following an initial assessment, all Navigational Incidents (those affecting or having the potential to impact upon navigational safety) are investigated further, from both a regulatory and safety perspective. Details of the incident, the investigation and outcomes are recorded in an incident database. Serious Incidents which have been investigated by the Harbour Master are summarised below:
On 23 November 2024 at approximately 02:00, an emergency services vessel hit a mooring buoy at high speed on the River Thames. The vessel departed its home berth near Waterloo Bridge at 01:53, tasked to an incident at Battersea Bridge. Whilst proceeding inbound to the incident location, the vessel collided with the lower mooring buoy at PLA Kirtling Barge Roads. The resultant impact holed the starboard side of the fibreglass hull at the waterline.
The Helmsman and two crew members did not suffer any injuries. Other assets were tasked to the original incident at Battersea Bridge. The vessel proceeded to Cadogan Pier where the crew could preliminarily assess the damage sustained. Upon finding a significant ingress of water, the crew started portable salvage pumps to extract the water. Additional emergency services vessels responded to assist the casualty vessel, with additional portable salvage pumps. Attempts to extract the water were unsuccessful. As a result, the casualty vessel was beached at Battersea Church Drawdock where the damage could be fully assessed.
Contributing Factors:
• The vessel was proceeding at maximum speed to the task at Battersea Bridge, for the majority of the passage up until the incident, the lifeboat was proceeding in excess of 40 knots and at the time the vessel made contact with the mooring buoy, they were proceeding at 41.1 knots. At this speed the Helmsman did not have sufficient time to take proper and effective action to avoid collision.
• The Helmsman was undertaking the operator’s structured competence-based training program to develop up to commander. As part of their development, it was agreed with the duty shift Commander they would take the role as Acting Commander for exercises and routine taskings. On the 23rd November 2024, the Acting Commander on the helm, had yet to complete the operator’s Local Knowledge module, which is a requirement of the Master of the vessel.
• Masters of certain vessels defined in Thames Byelaw 22 and Thames Byelaw 16 require a Local Knowledge Endorsement (LKE) due to the challenging conditions to navigate within this area. Navigating at high speed requires a high level of competency with local knowledge as reaction times are reduced, and the requirement to plan ahead is increased. Within the Local Operating Procedures of the vessel operator, there is a requirement for crew members to obtain the PLA LKE, which has not been enforced. The crew member on the Helm did not hold an LKE.
• Additionally, LKEs are required to be revalidated every 5 years by completing an Oral Exam with a PLA Examiner. This is to ensure the competence of the holder is maintained, taking into account changes of the tidal Thames within the LKE area. The commander previously held a PLA LKE, however, this was allowed to lapse in November 2023 due to the Commander no longer being full time with the vessel operator. Without a revalidation, it is unknown how up to date their local knowledge is.
• The vessel’s commander had the role of “seat 2” on the vessel for this tasking. This meant that they maintained communications with HM Coastguard and other emergency services. Due to wind noise which made communications hard to hear over the radio headset, the commander ducked down behind the console to listen. This resulted in them losing situational awareness, navigational oversight and prevented them from acting as lookout. This function could not have been performed by the crew member in seat 3, as their view was fully obstructed.
• As a vessel is rounding Westminster Boating Base inbound, the next visible reference point is the navigation lights of Victoria Rail Bridge arch 2. This course will navigate the vessel directly over the charted position of PLA Kirtling Barge Roads. With insufficient local knowledge to navigate further south and round the mooring buoys, combined with the buoys not being lit, difficult to identify and located in a dark area of the Thames with back scatter from shore lights, the temptation to navigate directly towards the navigation lights of Victoria Rail Arch 2 is significant.
Recommendations: The following recommendations have been issued to the PLA:
• The PLA are recommended to produce lessons learnt from this report, for distribution to appropriate audiences. • The PLA are recommended to consider developing a Certificate of Compliance scheme dedicated to emergency vessels under Thames Byelaw 16 as not to hinder their operation.
• The PLA is recommended to review its Memorandums of Understanding with the RNLI, Police, Fire Service and HM Coastguard.
• The PLA is recommended to review the positioning of PLA Kirtling Barge Roads to establish if the moorings should be removed or lit.
• The PLA is recommended to review unlit mooring buoys on the tidal Thames within high-speed zones, and identify the requirement for them to be lit based on similar traits of positioning and characteristics, including positioned on a bend in the river, positioned close to the edge of an authorised channel, poor back lighting conditions, and temptation for Masters to navigate on line of sight towards the buoy.
• The PLA is recommended to produce a policy for the installation of moorings, piers and other works, in and adjacent to, the authorised channel. The following recommendations were issued to the vessel operator:
• The vessel operator is recommended to ensure all Commanders, of all its stations on the Thames which operate and can be tasked to operate between Margaretness and Putney Bridge, hold a PLA LKE and maintain a regime of revalidation.
• The vessel operator is recommended to ensure, for its stations on the Thames which operate and can be tasked to operate between Margaretness and Putney Bridge, that all crew members who intend to act as Helmsman and exceed the speed limits of Thames Byelaw 16, hold a PLA LKE.
• The vessel operator is recommended to review the communications equipment used aboard their vessels which operate on the Thames above Margaretness, to ensure communications can be sufficiently heard whilst maintaining look out duties.
• The vessel operator is recommended to review their training procedures for helms and commanders on the tidal Thames, to ensure that trainers always maintains navigational oversight and control of the vessel. The following recommendation is issued to all Emergency Service Operators:
• Emergency service vessel operators are recommended to provide clear guidance to their Masters, ensuring they understand their legal obligations to maintain the safety of navigation and assess safe speed when responding to taskings and incidents.
Incident Description On 25 October 2022, an oil/chemical tanker departed from the berth in the early morning. While manoeuvring off the berth under pilotage, control of the ship was lost and it made contact with another fuel jetty at the site. The vessel’s starboard aft quarter was damaged in the accident, but there were no injuries. The resulting damage to the westernmost dolphin and a walkway, at the neighbouring berth caused the jetty to be taken out of commission for 2 months before being returned to service at reduced capacity until repairs were completed in September 2023. Contributing Factors:
The investigation concluded that:
• It was highly likely that the pilot was fatigued.
• It was highly likely the pilot was unfamiliar with the berth.
• The pilot had elected to sail without the support of a tug.
• Port of London Authority documentation on tug use had not been comprehensively updated to include a mandatory tug requirement for the berth, which was subject to the Control of Major Accident Hazard Regulations 2015.
• The vessel’s bridge team roles and responsibilities had not been allocated to best support the pilot during the manoeuvre. • The pre-departure master/pilot exchange was ineffective and unsuccessful, and challenges to decision-making did not result in changes to the departure plan.
• Parts of the Port of London Authority’s marine safety management system lacked clarity, and the management of pilot fatigue did not identify and control the risk of fatigue.
• The Port of London Authority had identified lessons from previous incidents, but these had not resulted in fully updated procedures and opportunities for capitalising on learning had therefore been lost.
• The Port of London Authority has taken numerous actions as a result of this accident that have included revisions to its safety management system, the withdrawal of out-of-date guidance and the introduction of qualitative reviews of pilotage plans. Recommendations: Recommendations have been made to the Port of London Authority to:
• Conduct risk assessments of high-risk berths (in conjunction with berth operators) • Review the risk and management of pilot fatigue
• Implement stop procedures
• Highlight to pilots the practices contained in the International Chamber of Shipping Bridge Procedures Guide. Recommendations have been made to the vessel operator to:
• Revise its fleetwide training in Bridge Resource Management and review the use of aids to navigation during pilotage. The International Chamber of Shipping has also been recommended to:
• Update its Bridge Procedures Guide regarding the assignment of roles and responsibilities during the master/pilot exchange.
Incident description
On the 29th March 2021 A container vessel was approaching the berth ready to commence a swing, preparing to berth port side to alongside the terminal when the vessel continued on a south west trajectory and went aground on the opposing side of the channel. The vessel was able to re-float back into the navigational channel with the assistance of tugs and berth safely. No damage, pollution or injuries were caused.
Actions Contributing factors
There are a number of factors which contributed towards the incident. In summary these were determined to include: The lack of a passage plan; Vessels speed which caused distraction to the Pilot; Lack of monitoring vessels position; Inappropriate use of vessel engines, rudder and positioning of tugs; Lack of corrective measures when the swing did not go to plan; Bridge team management was not effective.
All these factors contributed to the vessel coming to ground on the south side of the navigational channel, when there were no other mechanical or environmental reasons to affect the vessel.
Recommendations on the PLA Pilot to undertake time in simulator followed by a practical trip with similar vessel characteristics with a senior pilot to enhance learning experience.
Pilotage Manager to reissue updated version of OPL/2008/06 and re-word and reissue Operational letter OPL/2008/06 making clear the passage plan process during COVID restrictions.
Harbour Masters to Review best practice and processes for swinging large vessels and are recommended to commence periodical audits of pilot passage plans of all classes to determine if fit for purpose. They are also recommended to develop procedures to include initial actions post serious incident.
A copy of the investigation report should be circulated to all Pilots.
Recommendations for tug operator
Superintendent to ensure good positive communication is established & maintained between the Tug Master and Pilot to include confirmation of the securing positions & at all times during towage operations.
Actions taken by the VESSEL Onboard training to be conducted by Master for all bridge team members including lookout/helmsman. Training on “Roles/Responsibility of Bridge Team During Pilotage & Master/Pilot Relationship” to be conducted for all deck officers including Master. DPA to Re-iterate to fleet vessels the need to conduct detailed Master/Pilot Information Exchanges. DPA to share Incident report with entire fleet vessels for the lessons learnt.
Date
07/07/2019
Incident description
Vessel made contact with number 2 arch of Westminster Bridge, and was subsequently stuck under the bridge.
Actions
Vessel Operator to issue an Operations Memorandum to all crew members as a reminder of all engineering checks which are required, in addition to further educational discussions with the Master.
Date
17/06/2019
Incident description
Crew member injured arm whilst letting go aft spring during letting go operation. Paramedics attended and casualty (Ch. Mate) taken to hospital.
Actions
Note placed in POLARIS asking for the Harbour Master to be informed prior to the next call of the vessel following which the harbour service launch will visit the vessel and inspect it's mooring lines and give educational advice regarding the use of the ship's mooring lines as tow lines.
MAIB have been informed and followed up themselves receiving no further information to that provided by the PLA.
Date
06/06/2019
Incident description
Fatal man overboard from a recreational angling boat.
Actions
Assistant Harbour Master (Recreational) provided radar recordings and a statement to Kent Police to assist their investigation and report to the Coroner.
PLA to await the findings of the Coroner's Inquest and review to determine any appropriate actions.
Date
04/05/2019
Incident description
On the 4th May 2019 a Pilot tripped on the bridge of a vessel injuring arm resulting in Lost Time Accident.
Actions
PLA are to:
Remind ALL Pilots of the importance to report incidents in a timely manner.
PLA2
Circulate report to all pilots.
F1
Remind Masters for the need for a Good Bridge familiarisation briefing when an new or unfamiliar Pilot is on the Bridge.
F2
Review the highlighting of the raised platform to make more visible.
Date
22/04/2019
Incident description
Man overboard in an annual canoe race, resulting in a fatality.
Actions
The report recommends that the event organisers conduct a full review of the event risk assessment. This risk assessment is to identify all navigational hazards on the tidal Thames. All hazards are to be assessed and the appropriate level of mitigation is to be put in place before the next event. Further, a comprehensive communications plan to be submitted.
The Harbour Master's Department has taken action with the support of British Canoeing. A Safety Alert was published describing that serious incidents which have occurred in 2019 on the Thames Tideway resulting in paddlers being swept under industrial works barges on the Tideway.
The lessons regarding communications, risk assessment and fatigue are to be shared for all future events as appropriate.
Date
18/01/2019
Incident description
A Passenger rib with 8 passengers on board was navigating out bound on a charter to North Greenwich Pier. The Rib was navigating at speed and passed inside the Upper Outer Wing Buoy at which point the Master reduced speed to 26 knots before making contact with the Lower Outer Wing Buoy. The rib was launched into the air and on landing a number of passenger were knocked out of their seats, but remained on the vessel. The Master and Deckhand both made contact with the console screen causing facial injuries.
The incident was investigated by the MAIB and MCA Enforcement. The cause of the incident was a failure to maintain a proper lookout, but further issues were identified with the company’s SMS and Passage Planning.
Actions
The company are to:
1. Revise training including competencies required to keep an effective look out through the Type Rating for the Master and crew
2. Navigational Risk Assessment, SMS and Passage Plan to be updated to address high risk areas and identify hazards to navigation.
3. Review and update safety management system using the principles described in chapter 18 of the HSC Code, and relevant sections of the ISM code as detailed in the Technical Requirements for the issue of a CoC and submit to PLA for approval.
4. Review functions of the DPA and passenger counting and where that information is held to ensure compliance with the principles described in Chapter 18 of the High Speed Craft Code
Port of London Authority is recommended to:
1. Undertake a review of the PLA Navigational Risk Assessment for High Speed RIB operations in central London
2. Undertake a review of the Certificate of Compliance Technical requirements
3. Should the company meet the requirements for re- issue of a Certificate of Compliance, undertake a ‘For Cause' audit three months after the Certificate of Compliance is reinstated to ensure SMS has been fully applied to the operation.
The incident is also being investigated by the MAIB.
Enforcement Action:
MCA Enforcement leading on a prosecution under the Merchant Shipping Act.
Classification of navigational incidents in the Port of London
Navigational Incidents reported under the PLA's marine Safety management System are classified by severity as follows:
Minor Incident: Incidents, which do not affect persons and have a negligible cost implication (<£5K)
Serious Incident: Incidents which may involve slight/significant injury to persons and have a moderate cost implication (>£50K)
Very Serious incident: Incidents reported to the Board, which involve serious injury or fatality and have a serious/major cost implication (>£2M)
Incidents are categorised as follows:
- Contact
- Collision
- Grounding
- Loss of Hull Integrity
- Swamping
- Pollution
- Fire/Explosion
- Near Miss
- Inappropriate Navigation
- Navigational Hazard
- Breach of Byelaws
- Wash
- Breach of General Directions
- Floating Hazard
- Pilot Ladder Deficiency
- Vessel Equipment Deficiency
- Vessel Navigation Aid Deficiency
- Foreshore Incident
- Criminal/Malicious Damage
- Man Overboard
- Safe Access Deficiency
- Port Security Incident
- Other












